The fact that there was medication in Jonestown is undeniable: it was an isolated community in the Guyanese jungle that was attempting to be self-sufficient. To that end, Jonestown had its own doctor – Temple member Larry Schacht – as well as an entire group of individuals who worked, in one capacity or another, with the Jonestown Medical Facility. It was also a thriving community. In the last two years of its existence, for example, 33 babies were delivered within the encampment. The 1000 or so individuals who lived in Jonestown included 266 children under 16 – 258 who died and eight who survived – and approximately the same number of senior citizens. A functional Medical Facility and Medication dispensary was vital to the inhabitants and the viability of Jonestown as a population.
Those who worked in the Jonestown Medical Dispensary kept meticulous records of the medications that came into Jonestown, including how they were doled out. Many of these records were recovered after the tragedy and have been released through the Freedom of Information Act (FOIA). One section of this release – labeled J-1 – is a listing of the medications that were kept in the pharmacy, as well as the tracking and usage of each medication as it moved through Jonestown.
Last year, as I began my research into this portion of the FOIA records, I focused on the amount of Thorazine 100mg tablets, a highly powerful sedative used to treat severe schizophrenia, that was in the community. I also delved into how it was used to quash those who dared to dissent from the opinions of Jim Jones. This year, in a continuation of my research into the use of drugs in Jonestown, I’m focusing on the presence of barbiturates in Jonestown: specifically, the amount of 30mg tablets of Phenobarbital that were kept in the community. What makes barbiturates so interesting is the fact that Jones’ autopsy – conducted on December 15, 1978, nearly a month after his death – revealed that he had levels of Pentobarbital in his system that would be beyond toxic to the average person. The unspoken conclusion one can make from this finding: Jones had been taking the drug for years and had developed an extreme tolerance to it.
This article will explore the presence of 30mg tablets of Phenobarbital in Jonestown because it is the barbiturate with the most complete records in the medical log: among the subjects to be discussed will be the medical uses of barbiturates, how reasonable it was for the amount of Phenobarbital that was recorded as being in Jonestown to even be there for legitimate medical use, and how Jim Jones abused this drug.
Phenobarbital: Medical Data Regarding its Use by Adults and Children
 Phenobarbital has three uses for adults and one use for children who are prescribed it.
Phenobarbital has three uses for adults and one use for children who are prescribed it.
For adults, Phenobarbital can be prescribed as a “Daytime sedative” (30-120mg daily, divided into two-to-three doses), as a “Bedtime Hypnotic” (100-320mg, in one dose), and as an “anti-convulsant for individuals who have seizures” (50-100mg, two-to-three times daily).
For children who are prescribed Phenobarbital, it is to be used only for the prevention of “severe epileptic seizures.” Even with this single use, the individual dosage has other controlling factors, such as the age and bodyweight of the child. For children ages 1-5 years old, the dosage is 6-8mg, per kilogram of body weight, per day; for children ages 6-12 years old, the dosage is 4-6mg, per kilogram of body weight, per day. In children, all doses are to be given in one-to-two divided doses per day. In addition, elderly people – and there was a sizeable population in Jonestown – are often hyper-sensitive to the drug.
The side effects of the use of Phenobarbital vary. The most common one is drowsiness, but there are many others: agitation, confusion, abnormally low blood pressure, breathing difficulties, nausea and vomiting, lower body temperature, constipation, decreased heart rate, nightmares, difficulty in movement, anxiety/nervousness, dizziness and mental depression. It is also strongly suggested that a patient taking Phenobarbital not drink alcohol, as when the two combine, it’s a double whammy of depressant medication to the Central Nervous System (CNS). Children who take Phenobarbital may become unusually excited due to the fact that it’s common for younger individuals to be quite sensitive to the drug. Doctors who prescribe Phenobarbital to children are strongly encouraged to watch for indications that the medication is negatively affecting the behavior of the child.
But it isn’t just children who should be monitored closely by a doctor: overdosing on the medication is extremely dangerous, to the point that it can lead to unconsciousness and even death, because of the medication’s ability to suppress the CNS. It is therefore imperative that those who have any of the signs of a Phenobarbital overdose seek emergency medical help immediately. Signs of overdose are slurred speech, severe confusion, severe drowsiness, breathing problems, staggering, severe weakness and a slow heartbeat.
The long-term usage of Phenobarbital is discouraged for an individual unless it is an absolute medical necessity – such as severe and continued epileptic seizures – because the medication carries such a high potential for addiction, dependence, and tolerance. Tolerance towards barbiturates can be very dangerous and can get to a point where the usual dosage no longer works for an individual. In order to get the same effect that was achieved at a lower dosage when a patient first goes on a regimen of Phenobarbital, the dosage has to be increased. Over time, one’s body will continue to acclimate to higher and higher dosages. Eventually, an individual who has developed a tolerance to the drug will be able to take a dosage of Phenobarbital that is considered to be toxic to the average individual, merely to bring about the desired effect.
The Medical Records in “J-1”
The Medical Dispensary Records from Jonestown listed in section J-1 of the FOIA documents reveal that, during a seven-month period from April to October 1978, a great deal of Phenobarbital in the 30mg tablet form was kept there. The initial balance of pills “on hand” was 4,021. The first eleven notations in the log of pills leaving the dispensary don’t state where they were going, but from April 18th to May 26th, 968 pills were dispensed. Overall in the seven-month period for which we have records, a total of 3,859 pills (or 126,240mg) of Phenobarbital were given out in Jonestown. This is an incredibly large amount of pills for a group of roughly 1000 individuals.
A very intriguing – one might even say disturbing – notation in these records states that some of the Phenobarbital was sent to the Jonestown “nursery.” The “nursery,” located by the dormitories closest to the pavilion, according to research by Don Beck, was where the infants and young children were cared for while their parents did their assigned work. According to the medical records, Phenobarbital pills were sent to “the nursery” seven times in the ten weeks between July 14 and October 5, 1978, totaling 221 pills, or 6900mg.
We have previously discussed how Phenobarbital should be given to children solely for the treatment of “severe epileptic seizures.” Even if the notations of medications dispensed to the nursery were meant to include all the children of Jonestown – and for the sake of argument, using the population of 266 under 16 as those defined as children – would these amounts be considered reasonable? According to The Journal of Pediatrics, the incidence of epilepsy in children, is approximately 10.2 cases for every 1000 children. Extrapolating from that figure, one could expect no more than 2.71 children – rounded up to 3 – to have experienced epilepsy.
If anything, we should expect that number to be even lower, when we consider that the population of Jonestown was deliberately skewed to be healthier than a random population of 1000 people in the US. The applications for emigration to Guyana asked for detailed medical information, and anyone with severe mental or physical handicaps were denied permission to go. There is a possibility that one or two of the 33 children born in Jonestown had “severe epileptic seizures,” but it is certain that the Temple did not allow any children with a known history of such attacks to go to Guyana.
In short, it is impossible to make an argument that all of the Phenobarbital dispensed to the nursery could have been used for its intended medical purpose with children.
The Use and Abuse of Barbiturates by Jim Jones
No one is exactly sure when Jim Jones began to use barbiturates, but rumors abound that he had started to take them years before he moved to Jonestown. As a matter of fact, some believe that Jones’ constant use of sunglasses in the years leading up to his departure to Jonestown was a result of a sensitivity to light that he had developed due to his use of barbiturates. Whenever he started, though, there’s no doubt that he was taking barbiturates regularly, and that, by Jonestown’s final day, he had an extremely high amount of Pentobarbital in his system.
There is also no doubt that Jones’ use of barbiturates affected how he thought and acted while he was in Guyana. In his book Raven, reporter Tim Reiterman discussed Jones’ drug use this way:
The drugs – injectable Valium, Quaaludes, uppers, barbs, whatever he wanted – had taken hold of him. His voice, once so riveting, now sounded pathetic, raspy, as if he were very drunk or his tongue coated with peanut butter. Words collided with each other in slow motion. He would read from typed notes, but often not finish sentences. Sometimes, as he sat in West House [Jones’ private residence in Jonestown], barely gripping the army field phone that connected him to the radio room, he could not read at all.
Obviously, Jones was taking large doses of pharmaceuticals, to the point that he was barely functional at times, in the most basic of ways. It is terrifying to consider the ramification of ingesting so much medication: it was simply adding fuel to the fire to the deteriorating mental and physical state of the Temple leader.
Further evidence that Jones was heavily affected by his use of drugs – and barbiturates in particular – exists on many of the tapes of him speaking to Jonestown residents. In a number of tapes from the fall of 1978 as Jones reads the news – including Q216, Q267, Q285, Q210, and Q302 – he is heard slurring his words and/or sounding confused, both of which are clear indicators of barbiturate use and/or inebriation. In fact, these indicators – slurring of words and confusion – are two of seven that an individual may be suffering from a barbiturate overdose, and should seek immediate medical attention. One has to wonder if the people who were supposed to be personally monitoring Jones’ health were aware that he could have been in a desperate physical state.
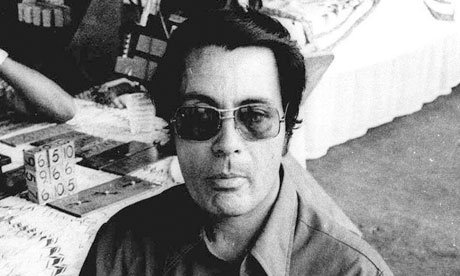 Jones’ abuse of barbiturates is visually apparent in the final TV interview he gave to the NBC reporters who had traveled along with Congressman Leo Ryan to Jonestown in November 1978. The Temple leader is clearly on drugs as he struggles to gather his thoughts and speak.
Jones’ abuse of barbiturates is visually apparent in the final TV interview he gave to the NBC reporters who had traveled along with Congressman Leo Ryan to Jonestown in November 1978. The Temple leader is clearly on drugs as he struggles to gather his thoughts and speak.
Just how much medication he was taking wouldn’t be known for another month, though. The autopsy of Jim Jones, conducted at Dover Air Force Base on December 15, 1978, showed that he was not just taking Phenobarbital, but that he had been ingesting barbiturates in various forms for such a long period of time that he had developed an extreme tolerance to the drug. Although Jones’ body had been embalmed and was in a state of advanced decay, the military personnel who performed his autopsy were still able to collect tissue samples of the spleen, liver, kidney and lung for toxicological examination, as well as the stomach and stomach contents.
The results were staggering: in milligrams per 100 grams of tissue, the stomach had 37.3mg, the liver had 5.7mg, and the kidney had 8.4mg. In comparison, the average level at which Pentobarbital is considered toxic for the stomach is 15mg per 100 grams of tissue, less that half the level in Jones’ stomach.
The autopsy notes:
The tissue levels of Pentobarbital are within the toxic range, and in some cases of drug overdose have been sufficient to cause death. The liver and kidney pentobarbital levels are within the generally accepted lethal range… The cause of death is not thought to be Pentobarbital intoxication because… tolerance can be developed to barbiturates over a period of time.
The other reason that the medical personnel did not attribute Jones’ death to drugs was the presence of the gunshot wound to his head, although the exact time of death, as well as a determination of whether the wound was inflicted by himself or someone else, could not be ascertained.
Nevertheless, it is obvious that Jones had developed an abnormally high tolerance to barbiturates, and no doubt it occurred over a period of years. Although it’s possible, it’s highly doubtful that his extreme tolerance developed in the last 18 months of his life that he spent in Jonestown; it’s far more likely that Jones had started taking barbiturates while he was still in the United States, and that the amount that he was taking ramped up once he arrived in Jonestown, culminating in the large amount of barbiturate found in his system during his autopsy.
Questions Posed by My Review of the Medical Records Listing Barbiturates in Jonestown
My examination of the records of barbiturates being in Jonestown leads to several conclusions, but it also leaves us with some crucial questions that need to be answered.
First of all, why was there so much Phenobarbital in Jonestown? For what purpose was it intended? We know people who applied for emigration to Guyana were screened for pre-existing medical conditions, and those who might have needed Phenobarbital for the control of seizures were denied permission to go to Jonestown. Why, then, would the pharmacy have brought in so many doses of the drug in the first place?
Secondly, there are notations in the Medical Records that some of the 30mg Phenobarbital pills were being put in what was called the “emergency kit.” That is the extent of the notation. We have no knowledge of what the “emergency kit” was, nor where it was kept or who was intended to use it.
A third, and most disturbing question raised by the Medical Records by far, is what did the notation in the records that Phenobarbital was going to the Jonestown nursery really mean? Were the records that 221 pills were dispensed to the nursery deliberately falsified to hide where the pills were really going? If so, where did the pills really go? Could they have been ferreted off to Jones’ private residence in Jonestown? Considering the meticulous record-keeping of the Medical Dispensary, this notation is quite odd at its most benign, and more likely as nefarious as it seems.
There is one final question which likely cannot be answered by any survivors and definitely will find no answer in the FOIA files: we know that Jim Jones abused drugs, likely as far back as during the Temple’s years in California, and we know that he died with toxic levels of barbiturates in his system; what we don’t know is who administered these drugs to him in Jonestown, and more importantly, how closely Jones himself was monitoring the dosage.
Jones was likely not the person to obtain the drugs from the pharmacy or the nursery. Like many of the other day-to-day tasks in his life, other people likely took care of this detail for him. There’s also a good chance that he wasn’t monitoring the pills he was taking – especially if he was already compromised – which leads to the possibility that one of the nurses or caretakers wasn’t merely an enabler for his drug abuse but actually the one who made the decision when and how often to administer the drugs. In other words, there’s a chance he wasn’t taking barbiturates, but rather was given them.
What would be the motivation for one of his trusted aides to do this? Consider the consensus of former Jonestown residents who survived the deaths that things ran a lot more smoothly when Jones wasn’t around, whether that was before he arrived, or when he was incapacitated during his time there. There are also indications that both his management style and his ideas for how to run Jonestown often got in the way of what needed to be done. For the sake of the smooth operation of the community, then, it’s possible that some people in his inner circle decided to reinforce his drug use without his knowledge, to keep him on a level of sedation that would allow him to do some things – read the news on the radio, attend a few meetings – but not others.
There is one document that supports this theory. On November 5, 1978, Annie Moore, one of Jones’ personal nurses, wrote a memo to Jim – with copies to Jones’ confidante Maria Katsaris and Annie’s sister Carolyn Layton – suggesting that another aide, Joyce Touchette, was plotting to “poison” their leader. While one interpretation of this memo is that Annie was slipping into the same paranoia as Jones himself, an equally plausible interpretation is that Annie could have been correct, but that the poison being administered to Jones were additional dosages of Phenobarbital beyond what was being “prescribed” for him or what he was already knowingly taking.
The FOIA records have helped me to add another piece of information to the puzzle of exactly what was going on in Jonestown. At the same time – as seems to be the case whenever one begins to investigate an element of life in Jonestown – my investigations have also raised new questions.
It may be that, with further digging through the FOIA records and greater research, some of these other questions will be answered. It is just as likely that these questions will never find resolution. Indeed, it is quite likely that the information that I’m seeking may be lost to the ages, extinguished forever along with Jim Jones, his inner circle, and the population of Jonestown on that horrible day of November 18, 1978.
(Bonnie Yates is a regular contributor to this website. Her previous articles may be found here. She may be reached here.)